When a person describes the feeling of bloating, they may or may not be aware of an increase in abdominal girth. The former is a symptom and the latter is a visible swelling and feeling of tightness of their skin or clothing along with discomfort. Often, patients will describe this as if a balloon has blown up in their abdomen and women often say that they look like they are several months pregnant. While bloating and distension often go together, they have different origins and possible treatments. Therefore, it is important to understand the differences.
Bloating vs. Distension
Bloating is a sensation, not a visible change in the waistline. It can occur for many different reasons: related to constipation, getting full after eating, or having disorders like functional dyspepsia or IBS. Bloating, like pain, is related to a combination of increased nerve signals arriving from the GI tract (i.e., due to visceral hypersensitivity) and/or ineffective regulation or control of the sensation by the brain. Changes in this brain-gut regulation, with the conditions noted above, can lead to more intense discomfort. As noted bloating can have different causes and treatment of the underlying condition can obtain relieve. For example using medications to improve constipation or antibiotics to reduce bacterial overgrowth or dysbiosis or neuromodulators to reduce visceral hypersensitivity in IBS can reduce this sensation.
For some people, this intense discomfort described as bloating or abdominal pain that often occurs after eating, can also trigger visible abdominal distension. The change in abdominal girth can be measured and seen by others as a swelling and change in belt size. Previously, this occurrence was frequently attributed to an increase of gas in the abdominal cavity with providers suggesting patients avoid swallowing air. However, several recent studies have used imaging to determine that gaseous distension such as from bowel obstruction or pseudo-obstruction occurs infrequently relative to most of the distension which actually is not due to increased gas. Instead the distension is called a visceral (gut) somatic (abdominal muscles) reflex that is triggered by the bloating sensation via the dysregulation of the brain-gut axis.
Dr. Drossman explains what abdomino phrenic dyssynergia is and shares treatment options via FaceBook live.
So, for example when eating a meal, food is eaten and it may stretch the stomach or intestines causing the bloating sensation. The sensation goes to the brain which has a reflex response to paradoxically move the diaphragm down into the abdomen and relax the abdominal wall muscles. This increases the pressure within abdominal cavity which pushes out through the relaxed abdominal wall leading to abdominal distention (see diagram). This is called Abdomino-phrenic dyssynergia. Abdomino-phrenic dyssynergia is a brain-gut reflex typified by bloating as a symptom and distension as a sign. It should be noted that bloating and distention can occur independently of one another. Not all people who experience bloating become distended and not all people with distension feel bloated.
Three treatment options can be utilized to treat Abdomino-phrenic dyssynergia including rebreathing techniques, central neuromodulators, and less commonly biofeedback with esophageal probes. The technique that our practice most often employs is to use central neuromodulators to reduce visceral hypersensitivity and improve brain regulation of the sensation which in effect raises the patient’s threshold for sensations like bloating and pain. By treating the brain-gut dysregulation, the sensation of bloating can be reduced and therefore the trigger resulting in distension does not occur or occurs to a lesser degree.
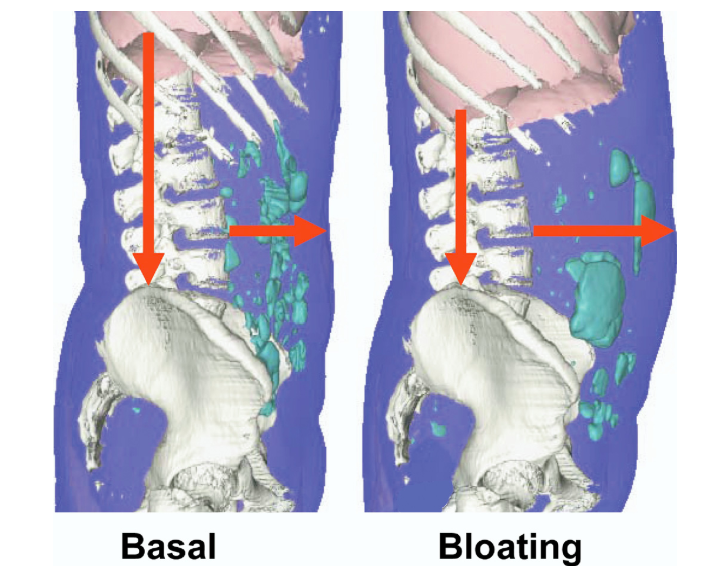
The above figure is taken from a paper in Gastroenterology demonstrates anterior abdominal wall protrusion and diaphragmatic descent during bloating compared with basal with only a small increase (by 22 mL) in gas content.1
References
Accarino, Anna, et al. “Abdominal Distention Results From Caudo-Ventral Redistribution of Contents.” Gastroenterology, vol. 136, no. 5, 2009, pp. 1544–1551., doi:10.1053/j.gastro.2009.01.067.